

Foot Morphology and Hallux Valgus Angle in Barefoot, Sandal-Wearing, and Shoe-Wearing Populations in Sri Lanka
PRELIMINARY REPORT — INTENDED FOR PEER-REVIEWED PUBLICATIONThis document presents preliminary findings shared for professional informational purposes. The manuscript is intended for peer-reviewed publication and is currently in preparation.
Abstract
This cross-sectional study examined hallux valgus angle (HVA) in adults aged 18–65 years in Sri Lanka, comparing habitually barefoot individuals, sandal/flipflop wearers, and conventional shoe wearers within a population likely to be more genetically comparable than in prior cross-cultural studies. Foot morphology was assessed using 3D scanning technology (Volumental). Barefoot individuals showed the lowest mean HVA values in both sexes. Group comparisons showed statistically significant differences between the barefoot and shoe-wearing groups (p < 0.001), with non-overlapping 95% confidence intervals. No significant difference was observed between the sandals and shoes groups. Effect sizes (Cohen’s d) were 0.78 for sandals vs. barefoot, and 0.91 for shoes vs. barefoot, the latter indicating a large effect. These findings suggest that habitual footwear exposure may be an important environmental correlate of hallux valgus angle variation within this population, and that the observed associations are unlikely to be fully explained by the demographic variables examined.
1. Introduction
The human foot is a biomechanically complex structure that, in its natural unshod state, distributes load across a broad plantar surface and maintains relatively straight alignment of the toes. The widespread adoption of enclosed footwear, particularly designs with narrow, tapered toe boxes, has been proposed as a major contributing factor to the development of forefoot deformities, most notably hallux valgus.2
Hallux valgus is one of the most prevalent musculoskeletal conditions globally, characterised by a lateral deviation of the great toe at the first metatarsophalangeal joint. It is estimated to affect approximately 23% of adults aged 18–65 years and is more common in women, a pattern consistently attributed to footwear characteristics rather than sex-based anatomy alone.3,4 Associated consequences include pain, reduced walking capacity, impaired balance, and lower quality of life, particularly in older populations.5
Previous comparative studies have shown that habitually barefoot populations tend to have wider feet, more even plantar pressure distribution,6,8 and lower rates of forefoot deformity than shod populations.1,7 However, a major limitation of this literature is that most comparisons involve populations of different ethnic backgrounds, making it difficult to separate the effects of footwear from those of genetic variation in foot morphology.9
Sri Lanka presents a rare opportunity to study these effects within a geographically and culturally related population. A substantial proportion of Sri Lankan adults are habitually barefoot or wear open flat sandals, while others, particularly in urban professional contexts, wear conventional enclosed shoes. This natural variation in footwear habits within the same population allows for a more controlled investigation of the relationship between footwear and foot morphology than cross-continental comparisons have previously permitted.
The primary aim of this study was to determine whether HVA differs systematically across habitual footwear groups — barefoot, sandals, and shoes — in a large Sri Lankan adult population.
2. Methods
2.1 Study Design and Participants
This was a cross-sectional observational study. Data collection took place in Sri Lanka during November 2023. A total of 1,071 individuals were scanned across multiple occupational groups, including tea plantation workers, fishermen, gem market workers, hotel staff, school teachers, police officers, and members of an Indigenous Tribe. Of these, 141 were excluded due to non-compliance with inclusion criteria, resulting in a final dataset of 930 participants aged 18–65 years. The diversity of occupational groups was deliberate, as these groups differ systematically in their habitual footwear use, providing a naturalistic footwear gradient within the same population.
Participants were recruited through convenience sampling across occupational settings selected to represent a broad range of habitual footwear use. Participation was voluntary; uptake among those approached was near-complete. Participants were included if they were within the specified age range and had no known congenital foot deformities or neurological conditions affecting foot posture.
2.2 Foot Morphology Assessment
Foot morphology was assessed using a validated 3D foot scanner (Volumental, Stockholm, Sweden), which produces a three-dimensional surface model of the foot from which geometric measurements are automatically extracted. The primary outcome variable was the hallux valgus angle (HVA), measured in degrees. Both feet were scanned; data from the left foot are reported as the primary outcome. Left and right HVA were strongly correlated across the full sample (Pearson r = 0.61, p < 0.001, n = 907), supporting the use of a single foot as a representative measure, though bilateral asymmetry was present in a subset of participants (difference > 5° in 36.7% of cases).9,18
2.3 Footwear Classification
Footwear habit was self-reported via a standardised questionnaire administered at the time of scanning. Participants were classified into three groups: Barefoot (no habitual footwear use), Sandals/Flipflops (primary footwear is open flat sandals or flipflops), and Shoes (primary footwear is conventional enclosed footwear). For the primary analysis, only participants reporting sandal or shoe use 5–7 days per week were included in the respective shod groups. Participants reporting sporadic footwear use (1–4 days per week) were excluded from the primary analysis. This yielded the following sample sizes: Barefoot n = 70 participants, Sandals/Flipflops n = 212 participants, Shoes n = 366 participants (left foot used for analysis). The questionnaire also captured lifetime shoe exposure through the question “How many years of your life have you been wearing shoes?”, recorded as decade intervals. This variable was used in a supplementary exploratory analysis.
2.4 Statistical Analysis
Group differences in HVA were examined using independent-samples comparisons and effect sizes were calculated as Cohen’s d. Mean HVA with 95% confidence intervals was plotted by footwear group and sex. Spearman rank correlation was used for the exploratory lifetime exposure analysis. Multiple linear regression was used to examine the footwear-HVA association after adjustment for age, BMI, and sex; the regression sample (n = 886) was smaller than the full dataset (n = 930) due to missing values on one or more covariates. The primary footwear group analysis (n = 648) excluded participants reporting sporadic footwear use (1–4 days per week). The lifetime exposure analysis (n = 906) excluded participants with missing questionnaire responses for that item. A sensitivity analysis additionally adjusting for occupational group was performed to assess residual confounding by socioeconomic and lifestyle factors. Data analysis was performed by Ales Jurca, PhD, Volumental AB, Stockholm.
3. Results
3.1 Sample Characteristics
Of the 1,071 individuals scanned, 930 were included in the final dataset following exclusion of 141 participants for non-compliance with inclusion criteria. The primary footwear analysis included 648 participants across three groups: Barefoot (n = 70), Sandals/Flipflops (n = 212), and Shoes (n = 366). The majority of participants were male (n = 649, 69.8%). Mean age was 43.1 years (SD 15.4, range 18–65). The largest occupational groups were Gem Market workers (n = 193), Hotel Staff (n = 182), and Tea Plantation Workers (n = 182).
Notably, the Barefoot group was older (mean age 50.9 years, SD 17.3) and had lower mean BMI (20.6, SD 4.7) compared to the Sandals/Flipflops group (age 46.1, SD 14.9; BMI 22.9, SD 4.8) and the Shoes group (age 36.6, SD 13.8; BMI 23.6, SD 5.0). The implications of these differences are addressed in the statistical analysis and discussion.
3.2 Lifetime Shoe Exposure and HVA
An exploratory analysis of the lifetime shoe exposure variable from the questionnaire revealed a modest but statistically significant positive association between cumulative shoe exposure and mean HVA (Spearman r = 0.17, p < 0.001, n = 906). Participants reporting zero years of shoe use showed the lowest mean HVA (2.3°), with a progressive increase observed with each additional decade of exposure, reaching 8.1° among those reporting more than 50 years of shoe use. This pattern is consistent with the primary footwear group findings. While this association is suggestive of a cumulative mechanical explanation for HVA development, it is not sufficient to establish one, and the self-reported exposure measure should be interpreted cautiously.
| Lifetime Shoe Exposure | n | Mean HVA (°) | Trend |
|---|---|---|---|
| 0 years | 130 | 2.3 | — |
| Up to 10 years | 144 | 4.8 | ↑ |
| Up to 20 years | 189 | 5.5 | ↑ |
| Up to 30 years | 128 | 5.9 | ↑ |
| Up to 40 years | 128 | 6.3 | ↑ |
| Up to 50 years | 117 | 7.7 | ↑ |
| 50+ years | 70 | 8.1 | ↑ |
3.3 HVA by Footwear Group
The primary finding is a progressive increase in mean HVA from barefoot individuals through sandal wearers to shoe wearers. Figure 1 shows the distribution of HVA values across the three footwear groups as a box plot, illustrating the systematic upward shift in both median and spread.
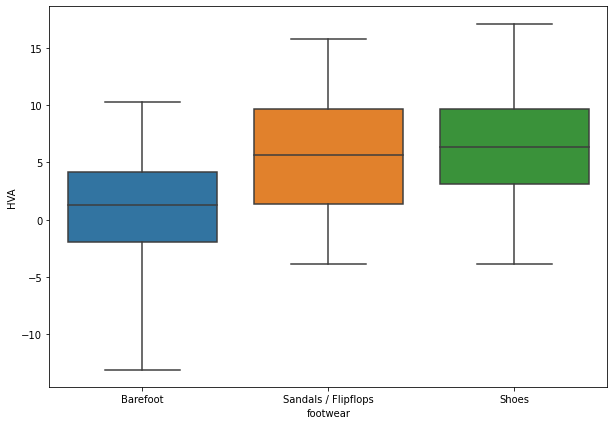
Figure 1. Box plot of HVA distribution by footwear group. Left (blue): Barefoot (n = 70 participants); middle (orange): Sandals/Flipflops (n = 212 participants); right (green): Shoes (n = 366 participants). The systematic upward shift in median and interquartile range across groups is evident.
Effect sizes (Cohen’s d) for pairwise comparisons were as follows:
- Sandals/Flipflops vs. Barefoot: d = 0.78 (approaching large effect)
- Shoes vs. Barefoot: d = 0.91 (large effect)
- Shoes vs. Sandals/Flipflops: d = 0.06 (negligible difference)
By convention, Cohen’s d values above 0.80 indicate a large effect size. The comparison between barefoot and shoe-wearing individuals therefore exceeds this threshold, indicating a potentially clinically relevant difference in HVA. The near-zero effect size between sandals and shoes suggested that these two groups were largely similar in terms of HVA, while both differed substantially from the barefoot group.
To examine whether the observed differences could be attributed to demographic factors, multiple linear regression was performed with HVA as the outcome and footwear group, age, BMI, and sex as predictors (n = 886). Sex was a significant predictor (β = +1.22° for female, p = 0.033), while age (β = 0.01, p = 0.49) and BMI (β = 0.02, p = 0.68) were not. The footwear group coefficients were not materially attenuated after adjustment, and remained highly significant: Sandals/Flipflops vs. Barefoot β = +4.42° (95% CI 1.69–7.15, p = 0.002), Shoes vs. Barefoot β = +6.83° (95% CI 3.97–9.68, p < 0.001). These results indicated that the footwear-HVA association was not materially attenuated after adjustment for age, BMI, and sex. A sensitivity analysis additionally adjusting for occupational group (n = 826) yielded similar results: Sandals/Flipflops vs. Barefoot β = +4.42° (p = 0.003), Shoes vs. Barefoot β = +7.37° (p < 0.001). It should be noted that in this sample, occupational group and footwear habit are inherently related — a police officer typically wears formal shoes, a tea plantation worker typically does not — making complete statistical separation of these variables impossible. The persistence of the footwear association after occupational adjustment nevertheless suggested the association was not explained by occupational differences alone.
| Group A | Group B | Cohen’s d |
|---|---|---|
| Sandals/Flipflops | Barefoot | 0.78 |
| Shoes | Barefoot | 0.91 |
| Shoes | Sandals/Flipflops | 0.06 |
3.4 HVA by Footwear Group, Stratified by Sex
Figure 2 presents the mean HVA with 95% confidence intervals by footwear group, stratified by sex, confirming that the primary footwear effect holds in both males and females.
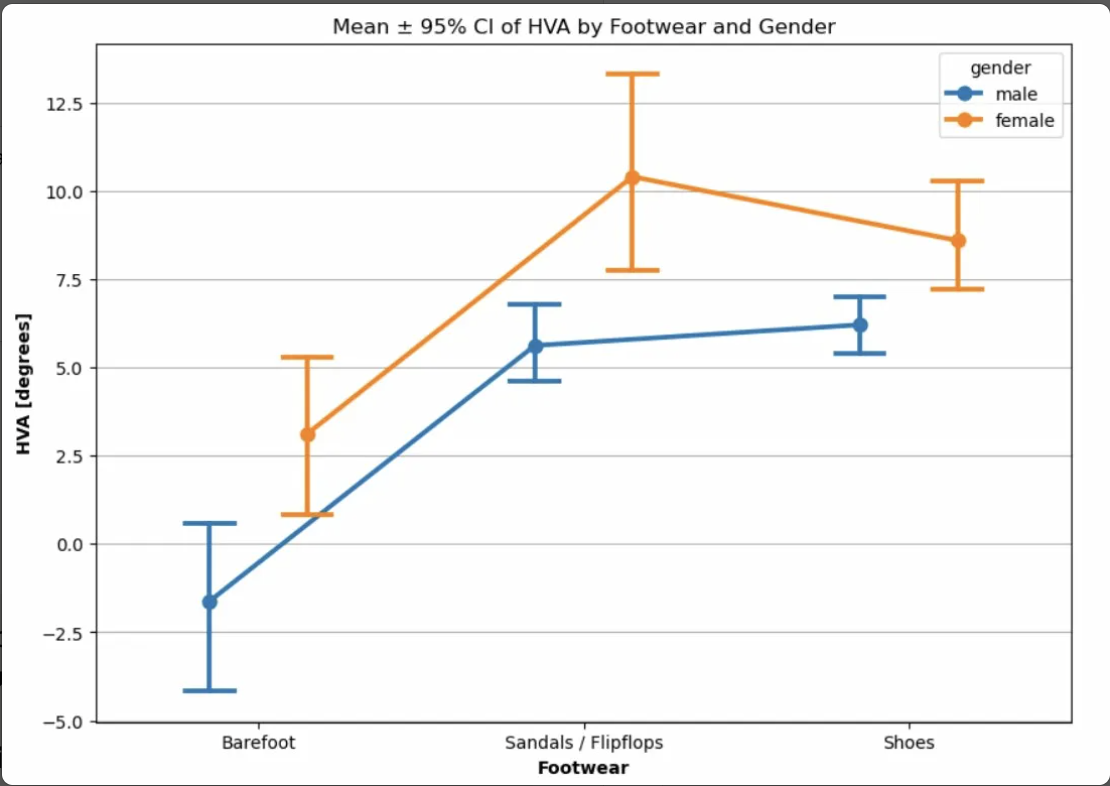
Figure 2. Mean HVA ± 95% confidence intervals by footwear group and sex (blue: male; orange: female). Data analysis by Ales Jurca, Volumental AB. Statistically significant differences are observed between the barefoot and shoe groups in both sexes (p < 0.001). No significant difference is observed between sandals and shoes.
- Barefoot individuals of both sexes had the lowest mean HVA values of any footwear group.
- Statistically significant differences were observed between barefoot and shoe-wearing individuals in both sexes (p < 0.001).
- There is no statistically significant difference in mean HVA between the sandals and shoes groups in either sex.
- Within the barefoot group, males showed lower mean HVA than females, an observation that warrants further investigation.
3.5 HVA by Occupational Group
Figure 3 shows HVA distribution across the nine occupational groups identified in the study. These groups differ substantially in their habitual footwear use, providing an additional dimension of comparison.
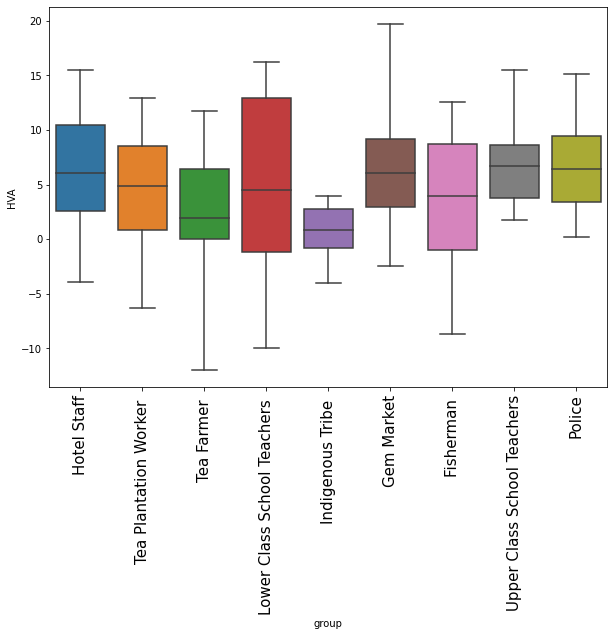
Figure 3. Box plot of HVA distribution across occupational groups in Sri Lanka (n per group shown in Table 2). The Indigenous Tribe shows markedly lower HVA values than all other groups. Upper-class school teachers and police show the highest values.
The occupational group data reflect the footwear gradient observed in the primary analysis. The Indigenous Tribe, the group with the most consistent habitual barefoot use, showed the lowest HVA values across all groups. In contrast, occupational groups with high conventional shoe-wearing prevalence, such as upper-class school teachers and police, showed the highest HVA values.
| Occupational Group | n (subjects) |
|---|---|
| Fisherman | 28 |
| Gem Market | 86 |
| Hotel Staff | 144 |
| Indigenous Tribe | 10 |
| Lower-class School Teachers | 18 |
| Police | 40 |
| Tea Farmer | 48 |
| Tea Plantation Worker | 144 |
| Upper-class School Teachers | 48 |
4. Discussion
The central finding of this study is clear and consistent: habitual footwear use is associated with a systematic increase in hallux valgus angle. Barefoot individuals showed the lowest HVA in both sexes, while conventional shoe wearers showed the highest. The effect size between these two groups (Cohen’s d = 0.91) exceeds the conventional threshold for a large effect, indicating a potentially clinically relevant difference in HVA.
A strength of this study is its design within a geographically and culturally related population. The majority of previous comparative work on barefoot versus shod populations has involved groups from different ethnic backgrounds. Such comparisons are inherently confounded by genetic variation in foot structure. By studying a population in Sri Lanka where barefoot, sandal-wearing, and shoe-wearing individuals coexist within the same population, we substantially reduce the genetic confounding that affects prior cross-cultural comparisons.
An important finding is that the observed association was not materially attenuated after adjustment for key demographic variables. The barefoot group was on average older (mean 50.9 years) and had lower BMI (mean 20.6) than the shoe-wearing group (mean age 36.6 years, BMI 23.6). Both older age and higher BMI might be expected to correlate with greater hallux valgus deviation. The fact that the barefoot group — despite being older and leaner — showed substantially lower HVA than the younger shoe-wearing group reduces concern about confounding by these factors. This is further supported by multiple regression analysis adjusting for age, BMI, and sex, in which the footwear group coefficients were not materially attenuated.
It should also be acknowledged that footwear habit may act as a proxy for broader lifestyle differences not captured in the present dataset, including physical activity level, terrain exposure, and socioeconomic status. While adjustment for age, BMI, sex, and occupational group did not materially attenuate the footwear association, residual confounding by unmeasured lifestyle variables cannot be excluded and represents a meaningful limitation of the cross-sectional design.
The near-zero effect size between sandal wearers and shoe wearers (d = 0.06) is an important and somewhat counterintuitive finding. One interpretation is that the critical variable is not the degree of shoe enclosure per se, but rather whether the foot is allowed to function completely freely, which only habitual barefoot use permits. It should be noted that the sandals/flipflops category encompasses a wide variety of designs. Our team observed that many sandal models feature a narrow anterior strap that constrains the great toe in a manner mechanically similar to an enclosed shoe toe box. This may have contributed to higher HVA in a subset of sandal wearers. It is also possible that the null finding between sandals and shoes may partly reflect exposure misclassification rather than true biomechanical equivalence, given the heterogeneity of sandal designs. Sandal subtype was not systematically recorded in the present dataset, and future studies should subclassify sandal designs to better characterise their mechanical contribution.7,10
Informal field observations suggested that individuals who had lived habitually barefoot into their twenties and only adopted conventional shoes in adulthood generally presented with better HVA values than those with lifelong shoe exposure. This was not formally analysed and should be considered hypothesis-generating only. If confirmed, it would suggest that the formative years of foot development may represent a particularly sensitive window, warranting investigation in future longitudinal studies, even if conventional footwear is adopted later.
The occupational group analysis adds ecological validity to the primary finding. Historical evidence supports a cumulative exposure pattern: archaeological analysis of skeletal remains in medieval Cambridge showed a marked increase in hallux valgus deformity coinciding with the introduction of pointed, fashionable shoes.11 The Indigenous Tribe in our study, likely to have the most consistent lifelong barefoot exposure, showed the lowest HVA values of any group. Upper-class school teachers and police officers showed the highest values. A sensitivity analysis adjusting for occupational group yielded similar footwear coefficients, suggesting the association is not explained by occupational differences alone. However, since occupational group and footwear habit are inherently linked in this population, complete statistical separation of these factors is not possible, and residual confounding cannot be excluded. Exploratory analysis of the lifetime shoe exposure data from the questionnaire further supports this interpretation, showing a progressive increase in mean HVA across decades of shoe use, from 2.3° in those reporting zero years to 8.1° among those reporting more than 50 years (Table 3), though the self-reported exposure measure should be interpreted cautiously.
In an exploratory post-hoc analysis, the barefoot group showed the highest bilateral symmetry between left and right HVA (r = 0.85), compared to the sandals (r = 0.56) and shoes groups (r = 0.62). This finding was not a primary outcome and should be considered hypothesis-generating only, but raises the question of whether unrestricted foot function may help preserve bilateral morphological symmetry — a question warranting formal investigation in future studies.
A sex-related difference was also observed within the barefoot group, with males showing lower mean HVA than females. As noted by the data analyst, the explanation for this pattern is not immediately clear, and it warrants specific investigation in future research.
These findings should be interpreted within their geographic and cultural context. The study was conducted in Sri Lanka, where the proportion of habitually barefoot adults is considerably higher than in most Western populations, and where occupational and lifestyle patterns differ substantially. Generalisation to other populations should be made with caution. These findings have direct clinical relevance. If conventional shoe design, particularly the narrow, tapered toe box, represents a potentially modifiable correlate of hallux valgus development, then footwear selection may be a meaningful target for prevention and early intervention in physiotherapy and podiatry practice.2,7,10
5. Limitations
- Cross-sectional design: The study establishes an association between footwear type and HVA. While multiple regression analysis shows the association was not materially attenuated after adjustment for age, BMI, and sex, a longitudinal or prospective design would be required to formally demonstrate that footwear change drives HVA progression over time.
- Small barefoot group: The barefoot group (n = 70) is considerably smaller than the sandals and shoes groups. While the group differences remain statistically significant after regression adjustment, the smaller sample increases uncertainty around mean estimates and limits sub-group analyses.
- Self-reported footwear habit: Classification was based on current self-reported footwear habit. The lifetime shoe exposure variable partially addresses this limitation by capturing cumulative exposure, and the progressive increase in HVA observed across decades of use supports the robustness of the primary findings.
- Sandal subtype heterogeneity: The sandals/flipflops group includes a wide range of designs with varying degrees of forefoot constraint. Future studies should differentiate between open flipflops and sandals with constrictive forefoot straps.
- Confounders not fully adjusted: While age and BMI were examined and found to be non-significant predictors of HVA, other potential confounders such as activity level, urban/rural setting, and occupational load were not formally adjusted for. While a sensitivity analysis adjusting for occupational group yielded similar footwear coefficients, occupational group and footwear habit are inherently linked in this sample, making complete separation of their effects impossible. Residual confounding by occupation, activity level, and urban/rural setting cannot be excluded and represents a meaningful limitation.
6. Conclusions
This study of adults aged 18–65 years in Sri Lanka demonstrates a significant and potentially clinically relevant association between habitual footwear type and hallux valgus angle, observed within a single geographically and culturally related population. Barefoot individuals consistently show the lowest HVA values, while conventional shoe wearers show the highest. The large effect size (Cohen’s d = 0.91) between these groups supports the hypothesis that footwear design, particularly features that constrain the natural alignment of the great toe, is consistent with a significant modifiable role in hallux valgus development.
The absence of a meaningful difference between sandal wearers and shoe wearers suggests that the critical protective factor is complete freedom of barefoot function. However, the heterogeneity of sandal designs, particularly the presence of constrictive forefoot straps in many models, likely reduces this comparison and should be addressed in future study designs.
These findings support clinical recommendations for footwear that respects the natural width and alignment of the forefoot, and highlight the value of early and sustained exposure to unrestricted foot function. An exploratory post-hoc observation of greater bilateral HVA symmetry in the barefoot group warrants further investigation in future studies.
Conflict of Interest
Ales Jurca is employed by Volumental AB, Stockholm, Sweden, which provided the 3D foot scanning technology used in this study. Rasmus Svärd and Melker Svärd are co-founders and co-owners of Wyde Footwear AB, a company that produces footwear designed with wide toe boxes. These relationships are declared in the interest of transparency. The study design, data collection, and analysis were conducted independently of these commercial interests, and neither Volumental AB nor Wyde Footwear AB had any role in the decision to publish or in the interpretation of findings.
Acknowledgements
We thank the community leaders, translators, and all participants in Sri Lanka who generously gave their time to take part in this research.
References
1. D’Aout K, De Clercq D, Aerts P. The effects of habitual footwear use: foot shape and function in native barefoot walkers. Footwear Science. 2009;1(2):81–94.
2. Ferreyra M, Nunez-Samper M, Viladot R, et al. What do we know about hallux valgus pathogenesis? Review of the different theories. J Foot Ankle. 2020;14(3):223–30.
3. Nix S, Smith M, Vicenzino B. Prevalence of hallux valgus in the general population: a systematic review and meta-analysis. J Foot Ankle Res. 2010;3:21.
4. Roddy E, Zhang W, Doherty M. Prevalence and associations of hallux valgus in a primary care population. Arthritis Rheum. 2008;59(6):857–62.
5. Menz HB, Roddy E, Marshall M, et al. Epidemiology of shoe wearing patterns over time in older women: associations with foot pain and hallux valgus. J Gerontol A Biol Sci Med Sci. 2016;71(10):1301–7.
6. Shu Y, Mei Q, Fernandez J, et al. Foot morphological difference between habitually shod and unshod runners. PLoS One. 2015;10(7):e0131825.
7. Gonzalez-Elena ML, Castro-Mendez A, Cohena-Jimenez M, Cordoba-Fernandez A. Relationship of the use of short footwear with the development of hallux valgus in a sample of Andalusian schoolchildren. Int J Environ Res Public Health. 2021;18:11244.
8. Mei Q, Gu Y, Xiang L, et al. Foot shape and plantar pressure relationships in shod and barefoot populations. Biomech Model Mechanobiol. 2019;19(3):1211–24.
9. Jiao Y, Dzeroski S, Jurca A. Analysis of hallux valgus angles automatically extracted from 3D foot scans taken in North America, Europe, and Asia. Ergonomics. 2023;66(8):1164–75.
10. Kinz W, Groll-Knapp E, Kundi M. Hallux valgus in pre-school-aged children: the effects of too-short shoes on the hallux angle and the effects of going barefoot on podiatric health. Footwear Science. 2021;13(1):29–42.
11. Dittmar JM, Mitchell PD, Cessford C, Inskip SA, Robb JE. Fancy shoes and painful feet: hallux valgus and fracture risk in medieval Cambridge, England. Int J Paleopathol. 2021;35:90–100.
12. Hollander K, de Villiers JE, Sehner S, et al. Growing-up (habitually) barefoot influences the development of foot and arch morphology in children and adolescents. Sci Rep. 2017;7:8079.
13. Kuhn J, Alvi F. Hallux Valgus. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
14. Klein C, Groll-Knapp E, Kundi M, et al. Increased hallux angle in children and its association with insufficient length of footwear. BMC Musculoskelet Disord. 2009;10:159.
15. Oh-Park M, Kirschner J, Abdelshahed D, Kim DJ. Painful foot disorders in the geriatric population: a narrative review. Am J Phys Med Rehabil. 2019;98(9):811–19.
16. Curtis R, Willems C, Paoletti P, D’Aout K. Daily activity in minimal footwear increases foot strength. Sci Rep. 2021;11:18648.
17. Puszczalowska-Lizis E, Zarzyczna P, Mikulakova W, et al. Influence of footwear fitting on feet morphology in 9-year-old girls. BMC Pediatr. 2020;20:349.
18. Jurca A, Zabkar J, Dzeroski S. Analysis of 1.2 million foot scans from North America, Europe, and Asia. Sci Rep. 2019;9:19155.